

{kind=link}
What if your body was quietly hoarding sugar instead of using it?
That’s essentially what insulin resistance is: your cells stop responding well to insulin, so sugar piles up in the bloodstream.
It’s common—about one in three U.S. adults has prediabetes—and the pancreas can only compensate for so long before blood sugar starts to climb.
In this post we’ll explain how insulin resistance works, why it matters for your heart and kidneys, and simple, practical steps you can try this week to nudge your body back toward normal.
Clear Breakdown of Insulin Resistance and How It Works
Insulin resistance happens when your muscle, fat, and liver cells stop responding well to insulin. That’s the hormone your pancreas releases to move sugar (glucose) from your bloodstream into cells for energy. Normally, a small amount of insulin is enough to unlock these cells and clear glucose from your blood. When cells become resistant, your pancreas compensates by making more insulin to achieve the same effect. This works for a while. But the pancreas can’t keep up forever.
Over months and years, the overworked pancreatic cells start to wear out. Insulin levels stay high, but blood sugar starts creeping up. That rising glucose marks the transition to prediabetes and, if left unchecked, to type 2 diabetes. Insulin resistance isn’t static. It fluctuates day to day and month to month, influenced by what you eat, how active you are, your stress levels, sleep quality, medications you take, and other health conditions.
In the short term, your body compensates well enough that you may not notice any symptoms. In the long term, persistently high insulin and rising glucose damage blood vessels and organs, increasing your risk for heart disease, kidney problems, and vision loss. Understanding how this progression works helps you see why early detection and intervention matter.
| Normal State | Insulin‑Resistant State |
|---|---|
| Cells readily absorb glucose when insulin binds to receptors | Cells respond poorly; glucose absorption is impaired |
| Moderate insulin levels maintain normal blood sugar | Pancreas produces high amounts of insulin to keep blood sugar in check |
| Blood sugar remains stable between meals | Blood sugar starts rising as insulin production fails to keep pace |
Insulin Resistance Mechanisms Explained Through Everyday Physiology

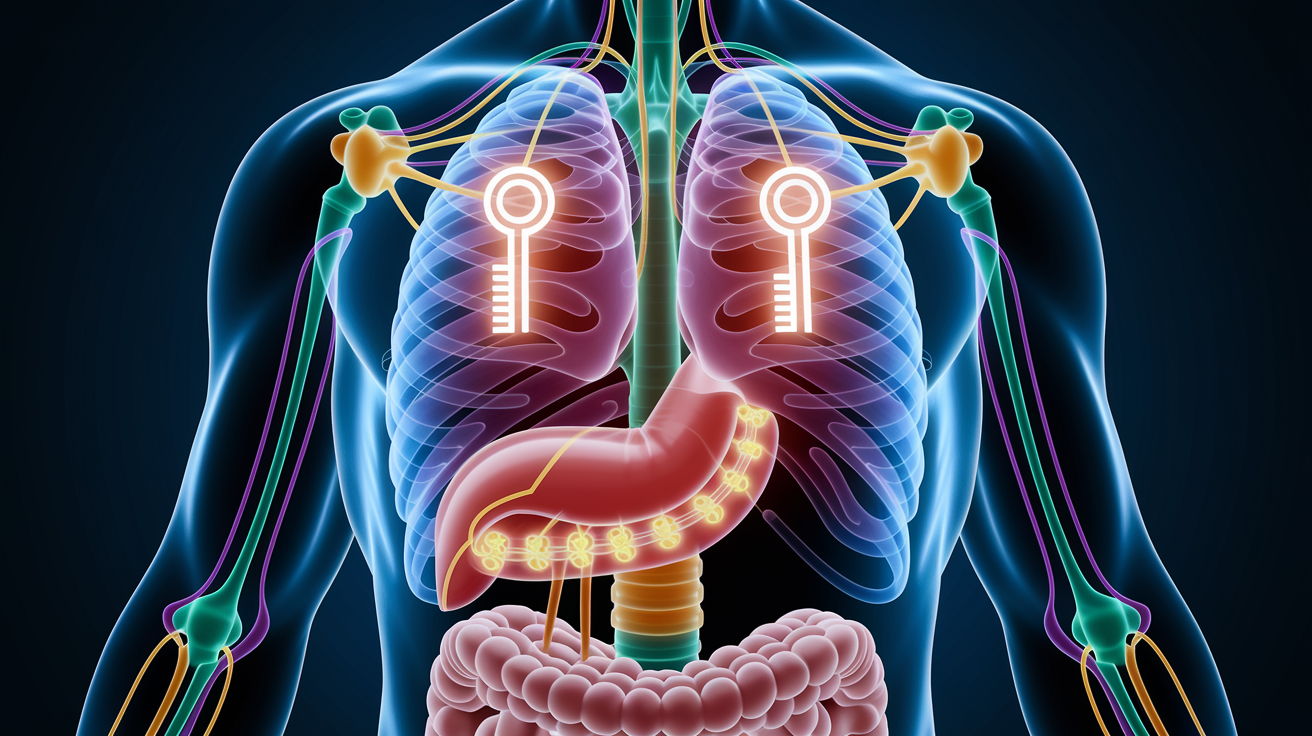
In a healthy system, insulin acts like a key. When you eat, glucose enters your bloodstream, insulin is released, and it attaches to receptor proteins on cell surfaces. That binding activates a cascade of signals inside the cell that tells specialized transporter proteins (called GLUT4) to move to the cell surface and open channels for glucose to flood in. This is how your muscles get fuel during exercise and how your liver stores extra glucose as glycogen.
When insulin resistance develops, the lock on the cell surface becomes sticky or jammed. Insulin still binds, but the internal signals weaken or stall. GLUT4 transporters don’t move to the surface efficiently, so less glucose enters the cell. Your pancreas senses the glucose piling up in the blood and tries to fix the problem by secreting even more insulin. For a while, flooding the bloodstream with extra insulin forces enough glucose into cells to keep blood sugar near normal. But the pancreas is working overtime and the cells remain unresponsive.
Insulin binds to cell receptors but triggers a weaker signal cascade inside the cell. GLUT4 glucose transporters fail to reach the cell membrane in adequate numbers. The pancreas compensates by producing higher‑than‑normal insulin (hyperinsulinemia). Over time, pancreatic beta cells exhaust and insulin production drops, allowing blood sugar to rise.
Insulin Resistance Risk Factors and Who Is Most Affected
Some risk factors for insulin resistance are fixed, others you can change. Age plays a role. Your risk increases after age 45. Family history matters too. If a parent or sibling has type 2 diabetes, your cells are more likely to develop resistance. Certain ethnic and racial groups face higher risk, including African American, Alaska Native, American Indian, Asian American, Hispanic or Latino, and Native Hawaiian or Pacific Islander communities. These populations often develop insulin resistance at younger ages and lower body weights than other groups.
Lifestyle and metabolic factors carry significant weight. Carrying extra body fat, especially around your abdomen (visceral fat), directly interferes with insulin signaling. Waist circumference is a quick screening tool: risk increases when your waist measures 40 inches or more if you’re a man, or 35 inches or more if you’re a woman, regardless of your overall body mass index. Physical inactivity compounds the problem because muscles are major glucose consumers, and regular movement keeps cells sensitive to insulin.
Medical history adds layers of risk. If you’ve had gestational diabetes during pregnancy, polycystic ovary syndrome (PCOS), heart disease, high blood pressure, or a stroke, your cells are more prone to resistance. Sleep disorders like sleep apnea starve your body of oxygen at night and trigger stress hormones that worsen insulin sensitivity. Chronic stress and poor sleep (less than 7 hours most nights) do the same. Certain medications can also nudge cells toward resistance: glucocorticoids (steroids), some antipsychotic drugs, and some HIV treatments.
Age 45 years or older. Family history of type 2 diabetes. Ethnic background: African American, Alaska Native, American Indian, Asian American, Hispanic/Latino, Native Hawaiian or Pacific Islander. Overweight or obesity, particularly abdominal fat (waist 40 inches or more for men, 35 inches or more for women). Physical inactivity or sedentary lifestyle. History of gestational diabetes. Polycystic ovary syndrome (PCOS). History of heart disease, high blood pressure, or stroke. Hormonal disorders such as Cushing syndrome or acromegaly. Medications including glucocorticoids, some antipsychotics, and certain HIV medicines.
Insulin Resistance, Prediabetes, and Diabetes Progression

Insulin resistance usually comes first, often years before blood sugar climbs into the prediabetes range. Prediabetes means your glucose levels are higher than normal but not yet high enough to meet the diagnosis of diabetes. Right now, more than 96 million U.S. adults have prediabetes. That’s roughly one in three people. And about 80 percent of them don’t know it because routine screening isn’t universal and symptoms are subtle or absent.
The progression looks like this: insulin resistance develops, the pancreas compensates by making extra insulin, blood sugar stays normal for a while, then the pancreas starts losing ground and glucose creeps up into the prediabetes zone (fasting glucose 100 to 125 mg/dL or A1c 5.7 to 6.4 percent). If nothing changes, pancreatic cells continue to fail and blood sugar crosses into diabetes territory. This is type 2 diabetes, which is fundamentally different from type 1 diabetes. Type 1 is an autoimmune condition where the pancreas produces little or no insulin from the start. Type 2 is rooted in insulin resistance, though people with type 1 can also develop resistance over time, especially if they gain weight or become less active.
| Condition | Typical Insulin Pattern |
|---|---|
| Insulin Resistance (no diabetes yet) | High insulin, normal or slightly elevated glucose |
| Prediabetes | High insulin beginning to fail; glucose 100–125 mg/dL fasting or A1c 5.7–6.4% |
| Type 2 Diabetes | Insulin production can’t keep up; glucose ≥126 mg/dL fasting or A1c ≥6.5% |
Symptoms and Early Warning Signs Related to Insulin Resistance

Insulin resistance is often silent, especially in the early stages when your pancreas is still compensating. You may not feel anything wrong. That’s why screening based on risk factors is so important. You can’t always rely on symptoms to warn you. When signs do appear, they’re usually subtle and easy to dismiss as normal tiredness or stress.
Common early indicators include feeling unusually tired after meals (especially carbohydrate‑heavy ones), strong cravings for sweets or starchy foods, difficulty losing weight around your midsection even when you’re trying, and darkened patches of skin in body folds, on the neck, armpits, or groin. That skin change, called acanthosis nigricans, is a visible marker of high insulin levels. As blood sugar starts climbing into the prediabetes or diabetes range, you may notice increased thirst, needing to urinate more often (especially at night), blurred vision that comes and goes, unexplained fatigue that doesn’t improve with rest, and cuts or infections that heal slowly.
Fatigue or sluggishness after eating, particularly meals high in carbohydrates. Strong cravings for sweets or refined carbs. Difficulty losing weight, especially around the waist. Darkened, velvety skin patches (acanthosis nigricans) in skin folds. Increased thirst and frequent urination. Blurred vision or slow‑healing cuts and frequent infections.
Diagnosing Insulin Resistance and Key Health Measurements

There’s no single standard test for insulin resistance that clinicians use routinely in everyday practice. Specialized research tools exist. Euglycemic clamp studies measure how well your body uses insulin in real time, and calculated indexes like HOMA‑IR (Homeostatic Model Assessment for Insulin Resistance) estimate resistance from fasting insulin and glucose levels. But these tests are complex, expensive, and mostly confined to research settings. In clinical care, doctors infer insulin resistance by looking at your constellation of risk factors and by checking your blood sugar directly.
The main screening tools are fasting blood glucose, hemoglobin A1c (which reflects your average blood sugar over the past 2 to 3 months), and sometimes a 2‑hour oral glucose tolerance test. The American Diabetes Association has clear cutoffs: a fasting glucose under 100 mg/dL is normal, 100 to 125 mg/dL signals prediabetes, 126 mg/dL or higher on two separate tests indicates diabetes. For A1c, normal is below 5.7 percent, prediabetes is 5.7 to 6.4 percent, and diabetes is 6.5 percent or above. An oral glucose tolerance test measures your blood sugar 2 hours after drinking a sugary solution. Normal is under 140 mg/dL, prediabetes is 140 to 199 mg/dL, and diabetes is 200 mg/dL or higher.
If you haven’t had your blood sugar checked in the past 3 years, now is a good time, especially if you have any of the risk factors listed earlier. Continuous glucose monitors (CGMs) are becoming more accessible and can show you real‑time patterns, helping you see how meals, activity, stress, and sleep affect your glucose throughout the day.
| Test | Normal | Prediabetes | Diabetes |
|---|---|---|---|
| Fasting Blood Glucose | <100 mg/dL | 100–125 mg/dL | ≥126 mg/dL (confirmed on 2 tests) |
| Hemoglobin A1c | <5.7% | 5.7–6.4% | ≥6.5% |
| Oral Glucose Tolerance (2‑hour) | <140 mg/dL | 140–199 mg/dL | ≥200 mg/dL |
Health Risks and Complications Linked to Insulin Resistance
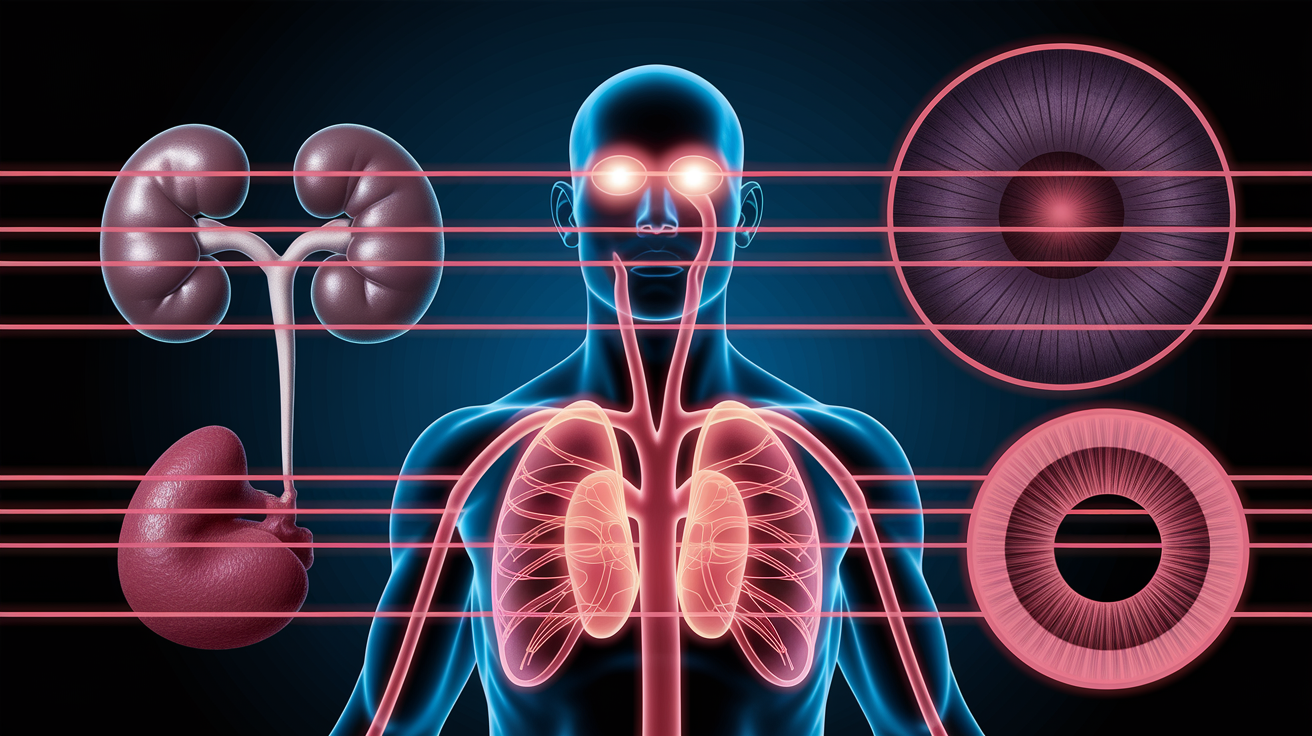
Left unchecked, insulin resistance sets off a cascade of metabolic problems that reach far beyond blood sugar. High insulin and rising glucose injure the lining of your blood vessels, accelerating atherosclerosis, the buildup of fatty plaques in arteries. This increases your risk of heart attack and stroke, the leading causes of death in people with type 2 diabetes. Your kidneys filter blood constantly, and chronic high glucose damages the tiny filtering units (glomeruli), which can lead to chronic kidney disease and, in severe cases, kidney failure requiring dialysis. High blood sugar also damages the small blood vessels in your eyes, leading to diabetic retinopathy, a major cause of adult blindness.
Insulin resistance doesn’t stop at glucose metabolism. It often comes bundled with other metabolic disturbances: high triglycerides, low HDL (good) cholesterol, high blood pressure, and excess abdominal fat. That cluster is known as metabolic syndrome. This combination amplifies cardiovascular risk. Your liver is also vulnerable. Insulin resistance promotes fat accumulation in liver cells, leading to nonalcoholic fatty liver disease (NAFLD), which can progress to inflammation, scarring, and cirrhosis. Chronic low‑grade inflammation and oxidative stress (cellular damage from unstable molecules) drive many of these complications, creating a self‑reinforcing loop of metabolic dysfunction.
Evidence‑Based Lifestyle Strategies to Improve Insulin Sensitivity

Exercise is the single most effective way to improve how your cells respond to insulin. Both aerobic activities (walking, cycling, swimming) and resistance training (lifting weights, bodyweight exercises) increase insulin sensitivity, and the benefits start within days. Aim for at least 150 minutes of moderate activity per week. That’s 30 minutes on most days. You don’t need to run marathons. Brisk walking that raises your heart rate counts. Strength training two or three times a week adds extra benefit because muscle is a major glucose sink, and building or maintaining muscle mass keeps your metabolism more flexible.
Weight loss, even modest amounts, can dramatically improve insulin sensitivity and reduce diabetes risk. Losing 5 to 7 percent of your body weight, about 10 to 15 pounds if you weigh 200 pounds, can cut your risk of progressing from prediabetes to diabetes by half or more, especially when combined with regular exercise. Weight loss works best when it’s gradual and paired with increased activity, because that combination preserves muscle while reducing fat. The quality of your diet matters too. Eating patterns that emphasize whole foods (vegetables, lean proteins, healthy fats, high‑fiber carbohydrates like beans and whole grains) improve insulin sensitivity more than diets built on refined carbs and added sugars. The Mediterranean diet, rich in vegetables, olive oil, fish, and nuts, has been repeatedly linked to better metabolic health.
Sleep and stress management are often overlooked but powerful levers. Sleeping fewer than 7 hours per night, especially if it’s chronic, raises cortisol (a stress hormone) and directly worsens insulin resistance. If you have sleep apnea, getting it treated can improve glucose control within weeks. Managing daily stress through regular physical activity, mindfulness, time with people you care about, or professional support helps keep cortisol in check and supports healthier eating and activity patterns.
Move for at least 30 minutes most days of the week. Walking after meals is a simple starting point. Include strength training at least twice a week to build or maintain muscle. Focus on whole foods: vegetables, lean protein, beans, whole grains, and healthy fats. Prioritize 7 to 9 hours of sleep per night and address sleep problems like snoring or apnea. Find daily stress outlets that work for you: exercise, social connection, or short breaks during the workday.
Medical Treatments Used for Insulin Resistance When Lifestyle Is Not Enough

When lifestyle changes alone aren’t sufficient to bring blood sugar into a safer range, medication becomes part of the plan. Metformin is the most commonly prescribed first‑line drug for prediabetes and early type 2 diabetes. It works primarily in the liver, reducing how much glucose your liver releases into the bloodstream between meals. Metformin also improves how muscle cells respond to insulin. It’s relatively safe, inexpensive, and has decades of evidence supporting its use.
For some people, especially those with obesity or significant cardiovascular risk, clinicians may consider newer classes of medications. GLP‑1 receptor agonists (like semaglutide or liraglutide) mimic a natural hormone that slows digestion, reduces appetite, and helps the pancreas release insulin more efficiently. These drugs often lead to meaningful weight loss, which in turn improves insulin sensitivity. Thiazolidinediones (TZDs) are another class that directly enhances how cells respond to insulin, though they’re used less often because of side effects like weight gain and fluid retention. SGLT2 inhibitors work by helping the kidneys excrete excess glucose in urine and have added benefits for heart and kidney health. Medication choices depend on your overall health picture, other conditions, and what you and your clinician decide together.
Prevention Strategies and Practical Tips for Long‑Term Insulin Health

Prevention is built on the same pillars as treatment: regular physical activity, a balanced diet, healthy weight, adequate sleep, and routine monitoring. If you’re at high risk (family history, overweight, sedentary, over age 45, or from a higher‑risk ethnic group), screening your blood sugar at least every 3 years (or sooner if your doctor recommends) catches problems early. Early detection means you can intervene before glucose climbs into the diabetes range. Research shows it’s possible to return blood sugar to normal with effective weight management and blood pressure control, especially if you act during the prediabetes window.
Tracking your progress helps you see what’s working. An A1c test every 3 to 6 months gives you a snapshot of your average glucose control. Continuous glucose monitors provide real‑time feedback, showing you how specific meals, activity, sleep, and stress affect your glucose hour by hour. Waist circumference is a simple home metric. Measure at the level of your belly button and track changes over time. Blood pressure and lipid panels (cholesterol and triglycerides) round out the picture because insulin resistance affects all these markers.
Practical prevention also means building sustainable habits rather than chasing perfect behavior. Plan balanced meals ahead of time, especially during busy or high‑stress periods like holidays. Eat consistently rather than skipping meals and then overeating. Walk for 10 minutes after lunch or dinner. It’s one of the easiest ways to lower post‑meal glucose spikes. If you take any medications (prescription or over‑the‑counter), ask your pharmacist whether they can affect blood sugar, and discuss alternatives with your doctor if needed. Prevention isn’t about perfection. It’s about stacking small, repeatable actions that keep your cells responsive to insulin over months and years.
| Metric | What It Indicates |
|---|---|
| Hemoglobin A1c | Average blood sugar over the past 2–3 months; target <5.7% to stay in normal range |
| Fasting Blood Glucose | Your baseline glucose after an overnight fast; goal <100 mg/dL |
| Waist Circumference | Marker of visceral fat; higher risk at ≥40 inches (men) or ≥35 inches (women) |
| Blood Pressure and Lipids | Cardiovascular health indicators often linked to insulin resistance; target normal ranges for both |
Final Words
You now know how insulin normally moves glucose into cells, how resistance develops, who’s at higher risk, common early signs, and the main tests clinicians use.
If you’re still asking what is insulin resistance, it’s when muscle, fat, and liver cells stop responding well to insulin, so the pancreas has to make more. That process can often be slowed with regular movement, better sleep, and steady eating habits.
Pick one small change this week—small wins add up.
FAQ
Q: What are signs of being insulin resistant?
A: The signs of being insulin resistant include feeling tired after meals, strong sugar cravings, stubborn weight gain, darkened skin folds (acanthosis nigricans), high triglycerides, and elevated fasting glucose or insulin on tests.
Q: How do you fix insulin resistance?
A: You fix insulin resistance by losing modest weight, adding regular aerobic and resistance exercise, improving diet (more fiber, whole foods, less added sugar), improving sleep and stress, and discussing medications with your clinician if needed.
Q: What is the difference between diabetes and insulin resistance?
A: The difference between diabetes and insulin resistance is that insulin resistance is when cells respond poorly to insulin and blood sugar is often still normal, whereas diabetes is high blood sugar when the pancreas can no longer compensate.
Q: Which foods cause insulin resistance?
A: Foods that cause insulin resistance include sugary drinks, refined carbs (white bread, pastries), highly processed foods, and diets high in saturated or trans fats; repeated excess calories and frequent ultra-processed meals raise long-term risk.